YAMOUT OPTICAL CENTER
|
YAMOUT OPTICAL CENTER |
|
Product
Optical historical |
Macular Degeneration The Retina The peripheral retina is composed of nine specific layers. Attached loosely to the outermost layer of the retina, are the retinal pigment epithelium (RPE) cells. These cells contain a high amount of pigment necessary for light absorption.* The next layer, known as Bruch's Membrane, is tightly bound to the RPE. Beneath this layer is the choroid, which contains a network of blood vessels, nerves, immune cells, and fibroblasts. Its function is to supply the RPE and outer part of the retina with nutrients. Encasing all of these layers is the sclera, which maintains the rigidity of the eye.
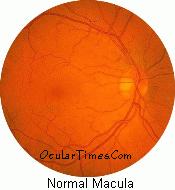
*Important Note: RPE cells support the function of photoreceptor cells (light-sensitive rods and cones) in the retina by providing essential nutrients and eliminating digested waste products. As part of the visual cycle, RPE cells convert vitamin A into a chemical that combines with a molecule found in rod photoreceptor cells to form rhodopsin. Rhodopsin is the visual pigment in rod photoreceptor cells that initiates 'phototransduction' -- the biochemical process through which photoreceptor cells convert an image into electrical impulses. The Macula All portions of the retina are responsible for sight, but only the macular region gives us our ability to distinguish fine central detail and color perception. The macular region contains a very different retinal configuration. In this region, the retina is thinned, especially towards the center of the macula (the fovea). The purpose of this foveal thinning is to permit greater light absorption. Another interesting aspect of the fovea is the absence of blood vessels over the photoreceptors. This contributes to the high degree of visual acuity found in the macular region because the light path to the photoreceptors is less hindered. Comparatively, the vascularization in the rest of the macula is very dense, creating the potential for many vascular related diseases.
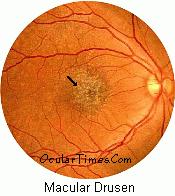
What Is Macular Degeneration? Macular degeneration is a progressive disease which afflicts approximately 11% of people in the United States over the age of 65. It is primarily a disease of the elderly, but can also be found in younger age groups. Aging, or systemic disease, causes the breakdown of retinal pigment epithelium cells in the macular region. As the disease progresses, central vision diminishes. It is believed that this breakdown may be due to a lack of nutrients being supplied to the region. Additional studies have found a genetic link to this disease. The Two Major Forms Of Macular Degeneration Dry Macular Degeneration
: (Neovascular) Wet macular degeneration is
associated with more sudden loss of vision. This form of
degeneration is characterized by macular hemorrhaging,
due to leakage or bleeding from abnormal vessels under
the macula. Vision loss can be rapid, due to the
disruption of blood flow to the layers of the macula
themselves. Eventually, these areas of blood and fluid
accumulation may develop into a dense mass of scar tissue
beneath the macular region. The most common symptom of macular degeneration is blurred central vision; noticeably worse when reading. In addition, horizontal lines may appear wavy and/or distorted. A useful way to detect macular changes is by viewing an Amsler Grid. During an eye examination, you may be asked to look at this grid. While staring at the grid's center dot, you will be asked if you notice any wavy, distorted, missing, or broken lines on the grid. Any one of these irregularities may indicate changes within the macular region of the eye. Your ophthalmologist or optometrist will be able to confirm any suspicions of macular degeneration during a dilated retinal examination.
Treatment For Macular Degeneration Unfortunately, there is no treatment today for dry macular degeneration. The sole recourse is to make lifestyle adjustments, learn to use optical devices that help to some extent, and hope the condition progresses slowly. For wet ARMD, two treatments are available, but both have major limitations. Both of the treatments involve a form of laser surgery that can be performed in an ophthalmologist's office, but just a small number of wet ARMD patients are candidates for these procedures, meaning that only a small minority of macular degeneration patients can be treated at all. Even then, neither procedure restores lost vision or cures the disease. · Laser Photocoagulation - This technique uses the heat of a laser to coagulate, or seal off, the leaky vessels that occur in neovascularization, preventing future bleeds from the treated vessels. Because it doesn't address the original cause or causes of neovascularization, this doesn't cure the disease. New vessels can continue to form, and the treatment almost certainly will need to be repeated. Another shortcoming of this technique is that it cannot be performed without destroying some of the healthy photoreceptor cells overlying the vessels. Moreover, if the leaky vessels are too close to the center of the macula, the surgery can't be performed at all because it carries a risk of destroying more central vision than it saves. · Photodynamic Therapy - In photodynamic therapy, a drug containing a light-sensitive dye is injected into an arm and allowed to circulate through the vessels growing beneath the retina. When the light of a laser is shown into the eye, the dye absorbs the light and the abnormal vessels are destroyed. The advantage of photodynamic therapy is that the weak vessels are pinpointed with more accuracy and considerably less heat is required from the laser (sometimes called a "cold" laser), which means less damage to nearby healthy cells. Still, photodynamic therapy has the same limitations as laser photocoagulation in the sense that it does not restore vision that has been permanently lost or treat the underlying cause by eliminating neovascularization. Researchers are beginning to explore the possibility that victims of wet macular degeneration may benefit from therapies developed to treat cancer. After all, scientists have long known that the growth of cancerous tumors involves the appearance of new vessels to provide the tumor with a blood supply. Some scientists are hopeful that the antiangiogenesis drugs that are beginning to show promise in stopping the formation of new vessels in cancer may be able to halt the neovascularization that underlies the development of wet macular degeneration. Earlier in 2000, a research team led by Peter Campochiaro at Johns Hopkins started human clinical trials of a new antiangiogenesis drug, called PKC 412, which has stopped new blood vessel formation in mice. A successful drug of this type may not restore lost vision, but, with early enough diagnosis, neovascularization could be stopped before any major bleeding and its attendant vision loss occurs. Another weapon that has long been used against cancer and may show promise for macular degeneration patients is radiation treatment. A clinical trial at Loma Linda University Medical Center, led by Les Yonemoto, has shown promise in treating wet AMD patients with a form of radiation called proton beam therapy. In this procedure, the eye is bombarded with proton particles, which can be targeted with great precision at abnormal vessels and lesions. The protons can destroy unwanted tissues with very little damage to surrounding healthy cells. So far, 65% of the patients treated with proton beam therapy have been able to maintain their same level of eyesight 18 months after the procedure, without the "collateral damage" that inevitably occurs with laser surgery. If this treatment can be used safely over lime, especially early in the diagnosis of wet AMD, it could spare many patients from major vision loss. Further studies indicate that diets rich in lutein and zeaxanthin (found in green leafy vegetables) may aid in slowing down the progression of the disease. For more information, please see Dietary Information. Below is a brief description of some of the latest procedures in use for the treatment of macular degeneration... · Submacular Surgery: An incision is made in the retina and instruments are used to remove abnormal blood vessels beneath the retinal surface. · Tissue Plasminogen Activator (TPA): Used to liquefy blood clots so that subretinal blood and fluids can be removed from beneath the retinal surface. · Retinal Translocation: In this procedure, the retina is surgically lifted and rotated away from the abnormal blood vessels; the vessels are then exposed to laser treatment without harming the center of the macula.
| |||||||||||||||||||||||||||
|
|