Conjunctivitis
Conjunctivitis
(inflammation of the conjunctiva) is a very common
disease that causes inflammation and swelling in the
tissues that line the inner lids and front of the eye.
This condition is often seen in contact lens wearers, but
can also be found in patients who suffer from allergies
and bacterial or viral infections. Conjuctivitis can take
on a variety of different forms, depending on the
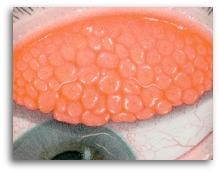
severity of symptoms. The example above illustrates a
form of conjunctivitis called Giant Papillary
Conjunctivits.
Signs and Symptoms
The most
common sign of conjunctivitis is a surface disruption of
the inner eyelids. On lid eversion, the conjunctival
tissue will appear injected (blood vessel dilation) and
inflammed. In more advanced cases, the inner lid will
have a cobblestone appearance. This cobblestone effect is
the result of papillary formations (inflammed tissue and
swollen vessels that give rise to "bumps") that
have developed in response to antigens. Other symptoms
may include...
·
Hyperemia of the conjunctival blood vessels (vessel
engorgement)
· Corneal epithelium disruption
· Excessive tearing, purulent
discharge, redness, itching, and foreign-body sensation
· Photophobia (light-sensitivity)
· Contact lens intolerance, with
blurred vision after insertion
Photo of
Severe Papillary Conjunctivitis

In soft lens
wearers, conjunctivits may develop as soon as three
weeks, or take as long as four years to manifest. In
rigid lens wearers, it typically appears after 14 months.
Causes
A critical
issue in formulating strategies to treat or prevent
conjunctivitis is to determine the specific causative
antigens involved in each particular case.
Contact Lenses
Protein
deposition on the surface of a contact lens is the most
common precursor for developing conjunctivitis. However,
protein on lenses of patients with conjunctivitis is
indistinguishable from protein on lenses of patients
without conjunctivitis. The antigenic stimulus could also
be one of a number of other potential lens contaminants,
such as lipids, calcium and mucus. Microorganisms such as
bacteria (and bacterial endotoxins) may also trigger the
problem.
The type of
plastic used to fabricate the contact lens may have an
antigenic role. In order to reduce the incidence of
contact lens induced conjunctivitis, many manufacturers
now provide lens materials that are more resistant to
protein, lipid, and calcium build-up collected from the
tear film.
Early
generation preservatives such as thimerosal and
benzalkonium chloride are known to have a causative role
in the development of conjunctivitis. For sensitive eyes,
it is recommended that preservative-free lens care
systems be used.
Mechanical trauma
Papillary
conjunctivitis of an apparently identical form to that
induced by contact lenses has been observed in patients
who do not wear contact lenses but whose tarsal
conjunctivae have been exposed to various types of
mechanical trauma, such as:
·
Plastic ocular prostheses
· Extruded scleral buckle (following
retinal detachment repair)
· Excessive cyanoacrylate glue used to
close a perforated cornea
· Protruding nylon sutures (following
corneal or lid surgery)
· Rigid contact lens embedded in upper
fornix
· Elevated corneal deposits
· Epithelialised corneal foreign body
(membranous growth over embedded foreign body)
Allergies
People can
develop seasonal, perennial and food allergies at any
age. Allergic reactions are triggered by the body's
immune system to protect the eyes from injury. The immune
system mistakes usually harmless substances (such as
pollens) for harmful foreign intruders (such as bacteria)
and over-reacts, producing allergy symptoms ranging from
mild to severe. The result can be considerable
discomfort, tissue damage and sometimes impaired vision.
To read more on how the body responds to allergens,
Treatment
Treatment
options fall into four categories:
Contact lens alterations
All soft
lenses develop deposits over time. Most of these deposits
can be removed by daily surfactant cleaning, but some
deposits such as protein gradually build up regardless.
Protein removal systems may slow the rate of protein
build-up but they do not prevent it. If protein
accumulation on the lens surface is determined to be the
cause, effective lens-related strategies include...
· Changing
to a lens material that resists protein build-up
· Changing to a lens material that
deposits less protein
· Changing to a rigid lens or
biocompatible material
· Replacing lenses more frequently
Cessation of
lens wear will usually result in an effective cure, but
such an option is generally met with little enthusiasm by
patients. In more severe cases (grade 3 or 4), ceasing
lens wear for a brief period of one week will enhance the
prospect of success of subsequent treatment. Similarly, a
reduction in wearing time in the early phase of treatment
will optimize the prospect for recovery.
A rigorous
approach to protein removal may alleviate contact lens
induced conjunctivitis. The introduction of protein
removal systems into the regimen of those patients that
do not use them, or an increase in frequency of usage
(e.g. from weekly to bi-weekly or even daily) may be
beneficial. This applies to both soft and rigid lens
wearers.
If
preservatives in contact lens solutions are thought to be
of actiological significance in a particular patient,
then the employment of preservative-free systems (some
hydrogen peroxide solutions fall into this category) may
alleviate the condition.
Improving ocular hygiene
Improvements
to ocular hygiene begin with improvements to personal
hygiene. Thus, routine thorough hand washing prior to
lens handling and regular face washing should mitigate
against developing conjunctivitis. Twice per day warm
compresses, followed by lid scrubs will help to remove
and express lid margin debris and bacteria.
Minimizing exposure
A first step
in treating eye allergies is to minimize exposure to
known irritants. Here are a few things that you can do
inside your home....
· Air
filtering
· Humidity regulation (to reduce mold
and mildew)
· Avoid perfumes, harsh detergents, and
carpet deodorizes
Pharmaceutical agents
A variety of
medications have been advocated for the treatment of
conjunctivitis and the provision of symptomatic relief.
Agents that act by stabilizing mast cell membranes, thus
preventing the release of inflammatory mediators such as
histamine, are helpful in the treatment of allergic
conjunctivitis.
In severe
cases of conjunctivitis, topical steroids aid in the
reduction of papillary hypertrophy and injection
associated with the condition. Unfortunately, long term
therapy with most topical steroids is contraindicated due
to potential side effects such as increased IOP and
posterior sub-capsular cataract formation.
Sources
* Portions of
text obtained from the Manual of Ocular
Diagnosis and Therapy. Pavan-Langston,
M.D., Little, Brown and Company, 1991.
|
