YAMOUT OPTICAL CENTER
|
YAMOUT OPTICAL CENTER |
|
Product
Optical historical |
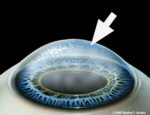
Corneal Transplant The cornea is the clear, living tissue on the very front part of the eye. Light passes through the clear cornea on its path toward the retina in the back part of the eye. Sometimes, the cornea is referred to as the "window" to the eye. Occasionally, either through disease or injury, the corneal tissue is damaged to a point where light can no longer effectively pass through it, resulting in reduced vision. When other methods of treatment have failed to save the cornea, or if vision has been lost in the affected eye, a corneal transplant procedure may be indicated. The procedure involves replacement of the damaged cornea with a healthy and clear donor cornea. Deciding When to Have a Corneal Transplant A corneal transplant, also known as a corneal graft, or as a penetrating keratoplasty, involves the removal of the central portion (called a button) of the diseased cornea and replacing it with a matched donor button of cornea. Corneal grafts are performed on patients with damaged or scarred corneas that prevent acceptable vision. This may be due to corneal scarring from disease or trauma. In this photo of a recent transplant, the fine V-shaped stitches can be seen clearly on the right side, though they extend all the way around the transplant. A common indication for keratoplasty is keratoconus. The eye-care practitioner must decide when to recommend keratoplasty for the keratoconic patient. This is often not a simple, straight-forward decision. Keratoplasty for keratoconus is highly successful; however, there is a long recovery period and a risk of severe ocular complications. A number of factors must be considered in deciding when to do a keratoplasty. One of the most important is the patient's functional vision. If the best acuity with their contact lenses prevents them from doing their job or carrying out their normal activities, a transplant must be considered. The actual measured visual acuity may be quite different for different patients. One patient may find that he/she can not do their job with 20/30 acuity while another patient may be very satisfied with 20/60 acuity. Very careful contact lens fittings are necessary before recommending a corneal transplant. One study found that 69% of keratoconics, most referred for transplant, could be successfully fit with contact lenses if special lens designs were used (Smiddy). Thus, prior to transplant every effort should be made to optimally fit the patient with contact lenses, especially if there is not significant corneal scarring affecting vision. However, a few patients become intolerant to contact lenses, and require a transplant earlier than otherwise would be necessary. If the patient has a large area of thinning, a very decent red cone or significant blood vessel growth into the usually clear cornea, called neovascularization, a transplant may be performed earlier than otherwise indicated by the visual performance, as these factors may require a larger than normal transplant button size and/or increase the chance of rejection if allowed to advance too far. The healing process following transplant is long, often taking a year or longer. The time from surgery to the removal of the stitches is commonly 6 to 17 months (Kirkness et al 1990; Troutman and Lawless 1987). The patient may be on steroids for months. Initially following surgery the donor button is swollen and even following healing the button is usually thicker than the corneal bed in which it rests. The photo on the left shows a thick white ring of scarring between the donated button and the patient's outer cornea. The white radial marks are where stitches were placed to hold the transplant in position. Graft rejection reactions occur in 11% to 18% of the patients (Kirkness et al 1990; Troutman and Lawless 1987). Signs of graft rejection include ciliary flush, anterior chamber flare, keratic precipitates, Khodaoust line and Krachmer's spots. Signs of graft rejection are reported to occur from 1 month to 5 years following surgery (Kirkness et al 1990). The rejection rate for bilateral grafts is higher than if only one eye is grafted. In the bilateral cases, when a rejection reaction occurs it is commonly in both eyes. If the second eye is to be grafted, there is usually a period of at least a year between grafts. If signs of rejection occur, aggressive treatment with steroids is begun. Usually the reaction is overcome and the graft remains clear. Over 90% of the corneal grafts are successful with some studies reporting 97% to 99% success rates at 5 and 10 years (Kirkness et al 1990, Troutman and Lawless 1987, Epstein). Large amounts of astigmatism are common following keratoplasty. One study found an average of 5.56 DC with a range from 0 to 17 D following suture removal (Kirkness et al 1990), with other studies showing an average of 5.4 DC (Troutman and Lawless 1987) and 4.5 DC (Smiddy). The patient's spectacle prescription may fluctuate for some months following surgery. Refractive changes and keratometry or corneal topography can be used to follow the healing process.
Contact Lenses After Surgery If a contact lens is required following keratoplasty it is customary to wait at least 3 months after the surgery and preferably until after the sutures are removed, which may be up to a year, before fitting contact lenses. Due to the irregularity of the cornea after transplant, soft contact lenses seldom give satisfactory vision. In addition, hydrogel lenses, scleral lenses and the SoftPerm lens may encourage vessel invasion into the graft. Therefore, rigid gas permeable corneal lenses are usually the lens of choice. Keratometer readings are seldom of any significant value in determining the base curve of the lens to use, but may be useful for baseline values to determine if any changes are occurring. Corneal topography with a computerized topographer can be of some value in determining the shape of the transplant and surrounding cornea. However, diagnostic lenses must be used to fit these eyes. Due to the size and shape of the button and the transition area between the button and the host cornea, it is often best to use a larger diameter lens to maintain lens centration. In the rare instance that a corneal transplant is placed off-center, rigid corneal lenses are nearly impossible to properly fit. In these few cases scleral or SoftPerm lenses may be the only viable option. Parameters of the lenses are assessed using the fluorescein pattern. The power of the final rigid lens is determined by an accurate refraction over the diagnostic lens. A lens material with good oxygen permeability should be used to minimize corneal swelling. The corneal transplant patient should be followed closely, especially during the first year or two following surgery to be sure corneal integrity is not compromised and that graft rejection is not occurring.
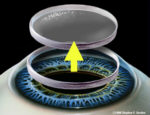
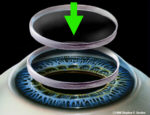
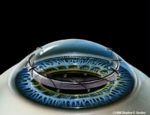
The Transplant Procedure This is an extremely delicate microsurgical procedure. The procedure first involves removal of a round, button-shaped shaped portion of the damaged cornea. This diseased cornea is removed with a special round cutting tool called a trephine. Then, a clear donor cornea, prepared to the same size, is replaced within the round opening. Finally, this donor cornea is stitched into place with extremely fine sutures.
Animation Of Procedure The surgery itself is painless and usually done on an outpatient basis. First, you are given eye drops or medication to help you relax. Then, a local or general anesthetic is used to prepare the eye. A patch is usually worn over the eye immediately following surgery. Other procedures may be performed at the time of corneal transplant surgery if necessary. Post-operative A corneal transplant takes many months to heal. Often, the stitches are not removed until six to nine months after surgery. During that time, medicated eyedrops are used to make sure the transplant heals properly. Possible Complications As with any surgical procedures, complications and/or side effects may occur. One of the risks of any transplant is the possibility of rejection. Our body is able to sense things that are not natural parts of it. The body's defense system tries to destroy these foreign tissues. Thus, it is natural for the body to try to destroy a transplant that is foreign because it comes from another person's body. This is the process called transplant rejection. If a corneal transplant rejects, it loses its clarity and swells. When rejection of the cornea occurs, the patient usually experiences the following:
Often, corneal transplant rejection can be stopped with medication, but rejection is always a possibility for the rest of the patient's life. If a transplanted cornea is rejected, another transplant may be done.
Donor Tissue Donor corneas come from healthy patients who donate their eyes after death. Ophthalmologists work closely with their local Eye Banks to obtain fresh tissue, which is kept in sterile preservative culture media until use. If you are interested in becoming an eye donor, you can simply check off a form when you get your next driver's license in most states. |
|
|