YAMOUT OPTICAL CENTER
|
YAMOUT OPTICAL CENTER |
|
Product
Optical historical |
Glaucoma Narrow Angle Glaucoma
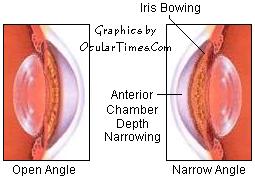
The "angle" refers to the physiological angle between the iris and the trabecular meshwork. When evaulating a patient for glaucoma, the physician examines this junction between the iris and the trabecular meshwork. An "open angle" means that the junction is wide enough to allow a normal flow of fluid through the trabecular meshwork. A "narrow angle" means that the junction is too narrow for fluid to flow normally, creating a risk of fluid backup which can cause increased eye pressure. As pressure rises, the iris may begin to bow forward, further restricting the flow of fluid and creating a shallow anterior chamber. · Narrow Angle Glaucoma (NAG) · Acute Narrow Angle Closure
Glaucoma (ANAG) Treatment of Narrow Angle and Angle Closure Glaucoma Medical treatment for Angle-Closure Glaucoma requires surgical intervention to reestablish a correct anatomical relationship between the iris and the trabecular meshwork. · Peripheral Iridectomy
In emergency cases of acute angle closure, the patient will be given several medications to help lower the IOP while in the hospital or clinic. These medications may be given prior to, or during, the peripheral iridectomy procedure in an effort to reduce significantly high pressure as quickly as possible. Peripheral iridectomy may be repeated if the desired IOP is not achieved after the initial procedure. Patients who undergo this procedure may experience an increased sensitivity to light, with mild glare noted with night driving. This is due to the increased amount of light entering the eye through the iridectomy opening.
|
|
|

 Laser iridectomy (also known as iridotomy)
consists of reestabishing a correct anatomical
relationship between the iris and drainage mechanism. A
small hole is made in the iris, either with a laser
iridectomy or surgical iridectomy. This hole allows for
excess fluid to drain, relieving the buildup of pressure.
Laser iridectomy (also known as iridotomy)
consists of reestabishing a correct anatomical
relationship between the iris and drainage mechanism. A
small hole is made in the iris, either with a laser
iridectomy or surgical iridectomy. This hole allows for
excess fluid to drain, relieving the buildup of pressure.